
We don’t (want to) talk about it…
Six full years have passed since the Great Threat—the Sars-Cov-2—has “struck” nearly all aspects of life for hundreds of millions of passengers on this planet. Six whole years later, it either feels like a century or has been pushed aside like a bitter, painful memory: we don’t want to talk about it (while we can talk about any small or big piece of nonsense).
Meanwhile, this “killer virus,” and indeed various naturally mutated, evolved, that is, more transmissible variants of it, continues to circulate. It circulates just as it would have in 2020, 2021, 2022, if there had been no “investment” in it, if it had not been advertised as the very harbinger of doom. It circulates indifferently, without causing a fuss greater than that of the common flu. Without feverish alarms, without a “war against the invisible enemy,” without militarization…
From a social, ideological (and ultimately political, in the full meaning of the word) perspective, it is rather particularly dangerous that the broad rejection remains unshaken even when comparing Sars-Cov-2 today with its ancestors six, five, or four years ago. Not a comparison of these viral forms themselves; a comparison of the social (and medical and mental) approaches surrounding them. A comparison of the (institutional) responses.
As if the overwhelming hygiene campaign that was unleashed six years ago had this rather unexpected “side effect”: the disappearance of memory and along with it the disappearance of interest in critical thinking, even when manipulation manages to become absolutely physical, cellular.
Could it be that this, the fact that manipulation through the hygiene terror campaign was absolutely physical, is the basis of the repulsion? Could it be, to put it differently, that the fact that “health” has become a kind of mass neurosis for a very large part of the citizens in the West makes criticism of the so-called “health industry” (as we will see in the following: industry promoting sickness) to a large extent self-criticism-of-broad-spectrum (and of psychological-emotional depth) and therefore repulsive?
Lost perhaps in the depths of collective amnesia, but it was an economist named Michael Grossman (director of the US “national bureau of economic research” from 19721 to 2020) who wrote something like a “gospel” in 1972 1 entitled On the Concept of Health Capital and the Demand for Health. In 1972 neoliberalism was still a marginal political-economic view. But Grossman did not hesitate:
… Over the last two decades, the view that individuals invest in themselves has become widely accepted in economic theory. At the theoretical level, increases in an individual’s knowledge base or personal capital are accepted as enhancing their productivity in the market sector of the economy where they generate their monetary gains, and in the non-market or household sector, where they produce goods that enter their daily functioning.
… The purpose of this study here is to construct a model for the demand for the commodity “good health”. The central premise of the model is that health can be considered as a durable capital stock that produces healthy time as a result. It assumes that individuals inherit an initial stock of health that deteriorates with age and can be upgraded through investment…
Grossman, described as a “pioneer” without hesitation, went so far as to calculate the “price” of various human organs in a “free trade” of human spare parts for transplants: “investment of the Self in improving his health”; and “sale of components due to necessity”.
The “idea” of the individual-capitalist-himself, initially equipped with two kinds of “fixed capital,” his education and his health, an idea of incorporating neoliberal rules into every individual and into the entirety of capitalist function / profitability, was not accepted immediately upon its emergence! But gradually, already from the late 1970s, during the 1980s, and with greater momentum from the 1990s onward, Western-type capitalist societies adopted this “model” into their everyday life without hesitation. And just as with any other commodity promotion, the promotion of the “good health commodity” became inextricably linked with the creation of new fears. Fears that are variations of the fear-of-death, fears of “social rejection,” “underperformance,” “imperfections,” etc. Neurotic fears, deeply rooted in the perceptions of millions of Ego-Capital after 2 or 3 generations voluntarily captive to neoliberal “truths.”
In 2020, this integration had become so deep and so commonplace that behaviorists and advertisers/propagandists of the “threat of death” (from the… “invisible enemy”… ) could easily manipulate the coarse but effective organization and guidance of the masses of citizens. Starting from the various forms of imprisonment of bodies (including their physical and intellectual ignorance: they had entrusted everything to the hands of the “experts”…) and proceeding to the “redemptive” acceptance, without doubts and concerns, of the “new technologies”, that is, the old-inspired and already failed therapeutic mRNA platforms of genetic engineering.
Rejections, willful, convenient ignorance, and misdirections into “police theories” are the oil that lubricates the gears of the total dominance of capitalist “guidelines” throughout daily life. In 1978, against the emerging view from its theorists of the “Chicago school” regarding health as “individual capital to be invested and returned / individual ‘profitability'”, the Alma-Ata Declaration proclaimed that health is a state of complete physical, mental and social well-being and not merely the absence of disease or disability. It was perhaps, from a historical perspective, the “last rifle” of a view that connected the health of individuals and social groups not simply and certainly not only with what the upcoming “health industry” would offer them, but with their emotional, intellectual, moral and ultimately social well-being. In 2020, such a view would be instantly condemned as… “fake news”…
We don’t want to talk about it anymore… Let each one of us deal with it alone.
Promotion of illness
Even today, despite the hundreds of thousands of victims of the “side effects” (despite the hundreds of thousands of “sudden deaths” and all the rest), the overwhelming majority of citizens cannot (and to a large extent do not want to) understand that it was not some accident, some wrong dosage in the generalized attack through the mRNA platforms of genetic engineering. Two major factors combine in this inability and, even worse, in this aversion. On the one hand, what we have already mentioned: the massive investment of Capital Egos over two generations in (individual) health, which meant investment and trust in health specialists. This is a condition whose age we can measure for Western societies gradually from the late 1970s/early 1980s onwards. On the other hand, in the deep, often paranoid trust in science (and in technology/science) and in its continuous progress – always for the benefit of people. Generally… This trust, regarding the “health sciences and techno-sciences,” began to be constructed already from the beginning of the 19th century.2
And yet what happened in 2020, 2021 and 2022 has a recognized (scientific) name and is scandalously well-known (not in demagoguery, only among the competent). It is called (in English) disease mongering which in Greek could be translated as promotion of diseases. “Disease promotion” is as old as, approximately, the steam engine; and yet “experts” and demagogues insist that there is no such issue. As for the masses; they prefer to ignore it.
As far back as 1992, journalist Lynn Payer, already known from the ’80s for her critical take on how pharmaceutical companies shaped the “culture” of illness and health, published a book titled Disease Mongers: How doctors, drug companies and Insurers are making you feel sick. Payer coined the term disease mongering, a term that was instantly accepted across various sectors, particularly in Western countries, sparking numerous studies, articles, and publications in medical journals, before the pharmaceuticals, insurance companies, and “medical associations” regrouped and fought back.
In a review of that book a few years later, one could read these interesting things as well:
You may believe that there are already enough diseases in the world and that no one would want to add to the diseases that we humans must face. However, there is a powerful industry in our society that works overtime to invent diseases and convince us that we suffer from them.
This effort is known as “disease mongering,” a term introduced by health sciences writer Lynn Payer in her 1992 book titled “Disease Mongering: How Doctors, Drug Companies, and Insurers Make You Feel Sick.” Payer defined disease mongering as “the effort to convince essentially healthy people that they are sick or slightly sick people that they are very sick.” This strategy has also been termed “corporate disease construction” by Ray Moynihan, Iona Heath, and David Henry in the British Medical Journal. “There is a lot of money to be made by telling healthy people they are sick,” they write. “Pharmaceutical companies actively participate in shaping the definition of diseases by funding and promoting them to both those who make the diagnoses and to consumers.”
The promotion of diseases began in 1879 with the invention of Listerine, which was initially considered a surgical antiseptic. It was named after the famous English surgeon Joseph Lister, who performed the first antiseptic surgical procedure. Soon, however, the inventors of Listerine, Dr. Joseph Lawrence and Jordan W. Lambert, were selling it in concentrated form as a floor cleaner and as a treatment for gonorrhea. In 1895 they began advertising it to dentists for oral care, and in 1914 it became the first over-the-counter mouthwash to be marketed in the United States.
Until the 1920s, the Lambert Pharmacal Company, the company that manufactured Listerine, was certain it had found a cure. Now all they needed was a disease. So, they invented one: “halitosis.” Before that time, bad breath was an unknown medical term that almost nobody had heard of. Advertisers began promoting Listerine as a treatment for this condition, which, they claimed, could reduce anyone’s chances of succeeding in love, marriage, and work. Soon, people across America were suffering from halitosis.
The trick was to inflate a common, everyday condition to the level of pathology, which, if not addressed, could undermine someone’s prospects for personal happiness and success. The advertisements created by Listerine merchants were mini soap operas, in which people risked social disgrace and failure, unless they used the product.
The merchants of Listerine improved the marketing techniques pioneered by 19th-century patented medicine manufacturers. Novelist Henry James was so annoyed by these swindlers that he called them “malicious.” His brother, Harvard psychologist William James, who is considered the father of American psychology, was also furious with them, saying that “the creators of these advertisements should be treated as public enemies and shown no mercy.”
Payer identified several disease promotion tactics. Among these:
- The implication that something is wrong with a physiological function and that it needs to be addressed;
- The medical indication for pain that does not necessarily exist;
- The definition of as large a percentage of the population as possible as suffering from the “disease”;
- The definition of a condition as a deficiency disease or as a hormonal imbalance disorder;
- The attraction of doctors to spread the message;
- The selective use of statistical data to overestimate the benefits of therapy;
- Promoting a commercially promoted therapy as risk-free;
- The deviation of a common symptom that could mean anything, presenting it as if it were a sign of serious illness.
These should easily be familiar; unless they are treated as “conspiracy theories,” which proves to be easier!
At another point in the same review, these are also noted:
… The approach to promoting diseases will not be easy. There is an almost unlimited amount of money that can be made from trading pharmaceutical therapies for diseases that exist mainly in the imagination, and there are strong economic, political and professional interests that desperately want this process to continue.
… Today, because religious comforts are no longer real for many people, death seems more terrifying, resulting in a frantic rush to use anything that offers better health and increased longevity.
… It has been said that one of the main ways in which we humans differ from other creatures is our desire to take a pill. Pharmaceutical companies know this.
The campaign for the construction of a disease to facilitate the trade of Listerine in the 19th century is certainly primitive compared to the later capitalist 20th or 21st century where no one prohibits (on the contrary) pharmaceutical companies from hiring sociologists, behavioral scientists, advertisers, journalists, and even deans of medical schools, “renowned” doctors of various specialties, commentators, influencers, so that both the declaration of a disease and its pharmaceutical treatment method have the characteristics and capabilities of total war dominance.
A small collection of studies published in 2006 may indicate the extent of morbidity construction, but – unfortunately – also the extent of success so far of circuits to replace religion (and the «fear of death» appropriately modified and packaged in thousands of different micro-packages / illnesses) in a completely profitable way:

For anyone who has doubts about whether the so-called “health industry” is in reality, without a second thought, an industry (designed) to produce illness, there is additional evidence – if there is room for such.
First that which was encoded as “the Gilead dilemma”:
There is a dilemma that very few people are willing to discuss publicly, but it must be addressed. When a condition is truly cured—or when a population is generally kept healthy—the long-term profits of providers, insurers, and pharmaceutical companies often decline. A clear example is Gilead’s Sovaldi (sofosbuvir). When Sovaldi appeared, it had a very high price and was heavily criticized by the media and politicians. However, it was also very effective and cured a very large percentage of the population with hepatitis C. This significantly reduced the patient population.
Although Gilead had significant short-term gains, it did not benefit from the existence of a sustained market since the disease burden decreased dramatically. Conversely, models of paid doctor visits and chronic illnesses produce recurring profits for stakeholders. Within this economic structure, managing chronic conditions—or managing health without reducing the patient base—can be more economically attractive compared to treating diseases or keeping populations truly healthy.
This is not a category for bad intentions – no organization wants to make less money and no one should expect such a thing. It exposes the structural problem of incentives in healthcare. The real question is how to redesign incentives so that treating diseases and keeping populations healthy have financially viable outcomes.
It’s not hard to understand that such “dilemmas” or, more accurately, the suggestion of a “need for ongoing illness” comes from the accounting departments (and representatives…) of private “healthcare” companies! From those who profit from sickness. Otherwise, a truly public health system would celebrate if the population it serves were healthy!
But a truly public health system could not be limited only to public health centers (primary care) and/or public hospitals. It should also be truly public throughout the entire healthcare sector, including research and the production of any medications.
No relation anywhere in the (western for sure) capitalist world! The situation is clearly indicated here, from Goldman Sachs (no relation to medicine or “health care”…) in an article from November 2018, about a year and a half before the construction of the terrible and horrific lethality of a generally indifferent “flu-type” virus:

«Is patient therapy a viable business model?» wonder the analysts at Goldman Sachs
One-day-out therapies for diseases are not something significant for businesses – more specifically, they are bad for their long-term profits – note analysts from Goldman Sachs on April 10 in a report for their clients from the biotechnology industry, which was first published by CNBC.
The investment bank’s report titled “The Genomic Revolution” poses the sensitive question to its clients: “Is patient therapy a viable business model?” The answer may be “no,” according to the following information.
The analyst Salveen Richter and her colleagues note:
“The ability to have ‘one and done’ therapies is one of the most attractive aspects of gene therapy, cell genetic modification therapies, and gene editing. However, such therapies have another side in terms of the revenue-to-time ratio compared to chronic treatments… Although this fraction has great value for patients and society, it could be a challenge for those developing genetic drugs who want a steady cash flow.”
As a real-world example, they cite the case of Gilead Sciences, which sells treatments for hepatitis C, with a cure rate of over 90%. In 2015, sales of these drugs by the company reached $12.5 billion. However, as more and more people were treated and there were fewer and fewer infected individuals to spread the disease, sales began to decline. Analysts at Goldman Sachs estimate that these therapies will generate less than $4 billion for the company this year.
“The rapid rise and fall of Gilead in relation to hepatitis C highlights one of the dynamics of an effective drug that cures a disease forever, but leads to the gradual depletion of the patient pool,” the analysts wrote. The report notes that diseases like common cancers – where “the pool of cases remains stable” – are less volatile for the industry.
To address the issue of sustainability in general, the report suggests that biotech companies focus on diseases or conditions that appear to be becoming more common and/or have a high frequency. It also advises companies to be innovative and continuously expand their range of therapies. “This can serve as a counterbalance to the declining trend in revenues from previous assets/therapies.” Finally, it observes that once such [genetic] therapies begin to yield results, they may open up even more investment opportunities for treatments targeting “diseases of aging.”
Cancers, “common” or not, and autoimmune diseases (we would add…) are a very good solution for the profitability of pharmaceutical companies (in general) and genetic-pharmaceutical companies (specifically): this is said without circumlocution. And since this is the case, the mass production of these (or any other) “chronic conditions” is also in the interest of the… interested parties.
Was this not done after the violent, mass imposition of mRNA platforms?
vertical alignment
Leaving aside the (almost non-existent under current conditions) exclusively and genuinely public healthcare sector, one could insist: doesn’t the interest of pharmaceutical companies and the entire (private…) medical circuit, including various medical specialties, conflict with the interests of insurance funds, and indeed, private insurance companies? Do we have here a version of capital versus capital?
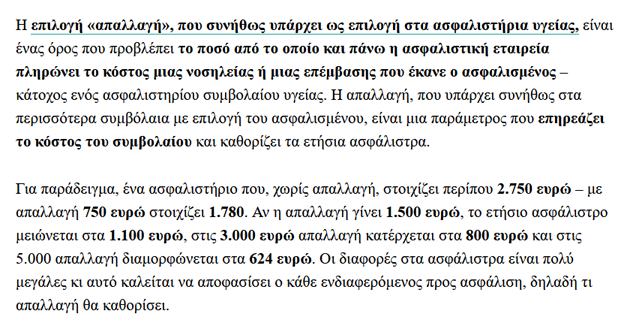
Indeed, this seems to have been happening for some years now… The expansion of morbidity increases the profits of both pharmaceutical cartels and private “providers,” while on the other side of the scale it puts pressure on both (public) insurance funds and private insurance companies. Which, at this stage, find an outlet in raising premiums; something that, however, cannot keep up with the frantic pace of the morbidity industry on one hand, and on the other is not always accepted by the insured. (For example: lifetime health and life insurance contracts in Greece fell from 711,000 in 2011 to 255,000 in 2023; while “compensation payments” (i.e., disbursements from private insurance accounting offices) between 2022 and 2023 increased from 212 to 227 million euros).
The solution to this “chapter versus chapter” drama is certainly not to prevent the disease industry! It is rather the merger! It’s about a “market” (“health”)…
On January 20, 2026, on the economic pages of the establishment’s “Kathimerini” there was this revealing report:
The Piraeus Bank group aims to change the operational model of the healthcare market, where insurance companies are limited to acting as passive intermediaries in their relationships with hospitals, paying the cost of hospitalization which they then pass on to insured members through high premium increases, for the acquisition of BioIatriki. Although the relevant discussions have not concluded, according to sources they are at an advanced stage, with the goal of acquiring the BioIatriki group, which includes two general clinics with a capacity of 266 beds and 70 diagnostic centers.
… The plan comes as a continuation of the acquisition of National Insurance. The goal, on one hand, is to reduce the high management cost of the health sector, which accumulates losses for the company, and on the other hand, to find ways for the effective development of operations, without the pressure created by the limited competition in the healthcare providers sector. The plan “connects” with the integration under the umbrella of the Hellenic Group – also belonging to Piraeus Bank – of Euromedica’s activities.
It is recalled that Hemithaea, which owns “Errico Dynan,” completed in June 2025 the acquisition of Euromedica’s clinics, creating a network of six general and obstetric clinics with wide geographical coverage in Greece.
It totals more than 1,200 secondary care beds, while over 2,500 employees and more than 3,500 collaborating doctors are employed in its clinic network. Hemithaea’s market share in the sector of general clinics stands at 6.6%, while the BioIatriki group holds a 24% share in the diagnostic centers sector and a much lower share of just 2.8% in the general clinics market.
From the side of insurance companies, the effort to operate as active health cost managers has been increasingly evident recently, with the latest move being Generali Hellas’s acquisition of Euroclinic, which operates two general hospitals (Euroclinic Athens and Children’s) with a total capacity of 175 beds. Additionally, the Interamerican group holds a shareholding relationship with Athenian General Clinic and, combined with the Medifirst polyclinics, has developed primary healthcare aiming for better control of hospitalization cases.
The European experience
In this way, insurance companies in our country are trying to follow in the footsteps of other European insurance groups, which no longer limit themselves to insuring risks, but acquire hospitals, clinics and primary care networks. This is a kind of vertical integration of the services provided in order to control the high cost of hospitalization.
Similar examples exist in Spain, where Sanitas (a subsidiary of Bupa) simultaneously operates as an insurer, owner, and manager of Sanitas Hospitales. It is indicative that it manages four private hospitals, 25 private medical centers, 17 advanced rehabilitation centers, a central laboratory, and a research institutional organization. In 2025, its portfolio expanded with the opening of the new Blua Sanitas Valdebebas hospital, while the construction of three new hospitals in Barcelona, Malaga, and the Arganda del Rey area of Madrid has been announced. The health insurer ASISA owns and manages the largest Spanish hospital network HLA, which has 19 hospitals and approximately 39 polyclinics, while Generali Spain has signed a 10-year strategic agreement (2023-2033) for its customers’ access to Sanitas’ extended network.
In the United Kingdom, Bupa, which has owned Cromwell Hospital in London since 2008, is a historically established insurer that is strengthening its direct-to-customer footprint by acquiring clinics, such as London Medical in 2024 and earlier the Blackberry Clinics & Smart Clinics units.
In Portugal, the country’s largest insurer, Fidelidade, acquired the Luz Saúde group in 2014 and remains the dominant shareholder with a vertically integrated health services offering.
In Poland, the largest insurance group, PZU, has built PZU Zdrowie as a provider network through acquisitions and mergers of clinics and polyclinics (e.g. Alergo-Med, Multimed-Elvita, CM Św. Łukasz), which, although it is not primarily “hospital-based,” like the Spanish or Portuguese examples, constitutes a clear form of vertical integration in secondary and primary care.
What does this privatization mean for the sickness industry? What does the chain of banks – private insurance – private “health” companies mean? The general idea is not to put a brake on disease mongering but, on the contrary, to make it even more profitable! This can be done in various ways: from the exclusion of various “coverages” by private insurance companies to the “exemption” through insurance contracts of a basic amount that the insured will pay (each time) from their own pocket.
However, most of these methods converge on the exploitation of customers’ personal data throughout the circuit, not only health data but also all the data each of these entities possesses: the bank (lots of data!), private insurance and healthcare structures, whether they are private companies or public organizations. By combining this data and creating a personalized “vulnerability profile,” disease promotion can advance to a “higher level,” personalized and accordingly paid.
A (age-related) field where this personalized disease promotion can be easily understood is minors/children. Even if an adult has the disposition to ignore a health “threat” concerning them, they will not do the same for their children. This type of campaign is already known from the “overdiagnosis” of attention deficit hyperactivity disorder (ADHD), childhood bipolar disorder – even from the medicalization of the slight stature.
And of course: anything that can be sold as a “minority” that has room for improvement; and the “defects in the dna”!
The anthropologist Marshall Sahlins argues that the belief in the unlimited nature of human desire is characteristic of the West and stems from the Christian notion of the “fallen man” as a victim who suffers. This, says Sahlins, has led to the popular idea of the individual as “an imperfect creature of needs and desires whose earthly life must tend toward the divinization of pleasure, indulgence, and the avoidance of pain.”
The history of professional advertising shows that at its heart lies exactly this assumption about the unlimited nature of desires. From many perspectives, advertising could be considered the systematization of the fear of imperfections and their inability to be overcome. Not coincidentally, objectively healthier societies fear illness more. It seems paradoxical, but the promotion of fears lies in suggesting what you still lack; or, if as a society you generally have more health, how much more you risk losing it.
When a telecommunications company appears as an “insurance agent” (in general but also health insurance) what else do you imagine if not “collection” and combination of personal data – secretly?
By leveraging individualism, pharmaceutical companies didn’t need to do anything more than convince each person of the value of consuming their products. The patient is a consumer. And with a skillful reversal, every consumer is (potentially) a patient. What can be called either medicalization or disease promotion falls from the tree of consumption like ripe fruit. And the construction of health threats is child’s play in the forests (or even jungles) of these individual, ambitious, and increasingly insecure trees. Pharmaceutical companies believe they are doing social work by equipping field doctors as well as consumers with suitable lenses to find—that-which-they-ignore-but-know-cannot-help-but-exist, a shadow of imperfection and inadequacy here and another one there. They secure their profits safely; and they claim that this is high art.
Ziggy Stardust

