
In a historical era when capitalist norms are expanding, sometimes “consensually” and sometimes violently, to control natural and social reproduction, with biotechnologies and governance in all their combinations, it would be unlikely for human pregnancy and childbirth to “escape” this trend. Technological “improvements” or “facilitations” here and there: the ideology that considers them “useful,” “innocent,” or even desirable has become entrenched in large segments of so-called developed societies…
The two short (translated) texts that follow touch briefly on developments in these issues. Written not in a spirit of strict militancy but rather as a cautionary note, they offer a first approximation of where “reproductive and enhancement technologies” stand today—and a reminder of the moral objections raised at a time when morality itself is out of fashion.
H.T.
it is too early for clinical trials in artificial wombs
A technology intended to help extremely premature babies raises issues of inequality and could at some point threaten parents’ rights to make decisions.
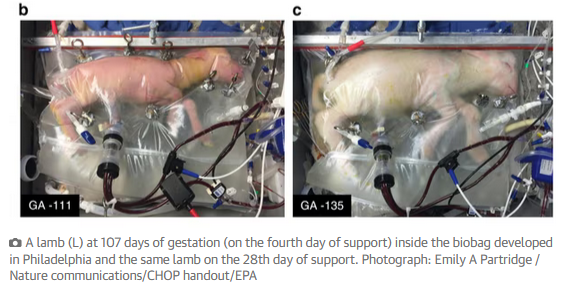
Artificial wombs are moving from the realm of science fiction to potential trials with extremely premature human babies. The potential benefits of this technology are great – however, with embryo rights becoming a political battlefield in the abortion debate, we believe that society must address the ethical and legal implications long before these clinical trials begin.
Globally, premature birth is the leading cause of death in children under five years of age. An artificial womb could provide extremely premature newborns with a mother-like environment, suspending the embryo in a flexible container filled with laboratory amniotic fluid. This innovation – which has so far only been tested on animals – could mitigate or even prevent the complications of premature birth, allowing the underdeveloped heart and lungs of the embryo to continue developing.
An advisory committee of the U.S. Food and Drug Administration is now examining whether to permit these first clinical trials in humans, despite the limited success of animal trials so far. Currently, from a bioethical standpoint, it is unclear whether animal models provide sufficient evidence to proceed to human trials. However, if the technology proves safe and effective one day, it could change the landscape. If this happens, what are the ethical and legal issues that concern us?
In order for the risks to be outweighed by the benefits of the artificial womb, it should be made available to embryos that often do not survive using current technology—with incubators, surfactant, and oxygen, among other things. Embryos at 23 weeks or more of gestation tend to do well with current technology. But embryos under 23 weeks do not make it. The decision to use an artificial womb will place enormous pressure on prospective parents, who will have very little time to make difficult decisions regarding participation in the trial, to the point where their ability to meaningfully consent, with full understanding of the risks involved in participation, is essentially compromised.
Decision-making at the limits of fetal “viability” is already ethically and clinically very complex, as clinicians and prospective parents weigh various possible outcomes. Viability is a difficult target, where outcomes are almost impossible to predict, with or without this new technology. Without clear regulatory protection of parental autonomy in making these decisions and without better animal studies describing potential benefits, artificial wombs could worsen an already burdened landscape, pressuring and limiting decision-making by prospective parents.
Behind these concerns lies the ongoing ethical debate regarding the moral status of the embryo and attempts to achieve a “scientific” determination of when an embryo acquires “full” moral status or even personhood. Within this complex framework, people can reasonably disagree. Most national medical societies strongly encourage leaving decisions regarding pregnancy termination, mode of delivery, and recovery parameters to pregnant individuals and their medical teams. If artificial wombs promote restrictive regulations that limit decision-making by parents and clinical physicians, serious ethical concerns will arise.
Subsequently, the technology will expose pregnant women to significant risks, with—so far—only hypothetical benefits for their embryos. Most of today’s applications of the technology require a cesarean section, which is far more dangerous at earlier stages of pregnancy than a standard cesarean and could jeopardize future fertility. Achieving truly informed consent, given all these pressures and complications at a literal “do-or-die” moment in reproduction, could be impossible.

Moreover, what happens if a pregnant person declines this option? Artificial wombs could be used in ways that restrict reproductive freedoms. The anti-abortion movement already supports cesarean sections—even over the objections of pregnant patients—to optimize outcomes for the baby. In a political climate where reproductive rights are curtailed in the name of protecting embryos, safe and effective artificial wombs could be used to argue that the embryo not only has a right to life, but also a right to any available medical care. Such an argument could promote legislation imposing dangerous surgical interventions despite the pregnant person’s objection. With current laws defining the status of personhood in various American states, this is a real possibility.
From the perspective of reproductive justice, this technology is unlikely to be equally accessible. While the global under-five mortality rate continues to decline worldwide, children in sub-Saharan Africa still have the highest mortality rate in the world, with 74 deaths per 1,000 live births – 14 times higher than in Europe and North America. Many of these deaths are associated with premature birth. Clinical trials with artificial wombs, let alone their use in clinical practice, are unlikely to be available where they are needed most.
Finally, looking toward the distant future, questions arise regarding the possibility of using artificial wombs at the beginning of pregnancy. Most researchers today believe that using this technology in the early stages of the first trimester, when most abortions occur, would be impossible. However, science is always innovative, and one can imagine a dystopian future in which it would be possible to tell a pregnant person: if you do not wish to continue this pregnancy, we can separate you from the embryo and transfer it to an artificial womb.
What would such a scenario mean for prospective parents? Would they still be considered the legal parents of the entity in the artificial womb? Or would there be a presumption in favor of adoption? Would the artificial womb make both genetic parents equal decision-makers, since the embryo is not located in the body of only one of them? Or would both lose their authority, leaving decision-making in the hands of regulatory authorities? How would current clinical norms regarding decision-making for premature infants translate into this framework?
While artificial wombs promise much, advancing the first trials in humans – lacking clear evidence of potential benefit – poses significant risks of limiting the reproductive rights of future parents.
Source: www.scientificamerican.com/article/it-is-too-soon-for-clinical-trials-on-artificial-wombs/
Date: May 31, 2024
Translation: Harry Tuttle
super babies
The latest fertility technology calls on parents to select their baby’s characteristics as if they’re shopping at Whole Foods.
The “pronatalist” parents [pronatalism: an ideology that promotes reproduction as the supreme moral obligation and treats women as reproductive machines], such as Simone and Malcolm Collins, want it all: optimized babies – many babies.
To achieve this goal, the couple from Pennsylvania uses an emerging technology known as preimplantation genetic testing for polygenic disorders, or PGT-P, to select embryos during in vitro fertilization. The Collins proudly identify as autistic, so they do not exclude embryos that are considered to carry a predisposition for autism. They select for traits such as IQ and deselect those they call “traits associated with mental health.” Selecting embryos for desired and undesired traits, the Collins say, is the first step toward achieving their goal of “gentle parental care.”
The family is part of the next boom that will hit Silicon Valley: fertility technology for producing “super babies.” High-profile tech entrepreneurs, such as Sam Altman, CEO of Open AI, Anne Wojcicki, CEO of 23andMe, and billionaire entrepreneur Peter Thiel, CEO of Palantir, are backing emerging companies with names like Orchid Health, Gattaca Genomics, and Genomic Prediction.
These companies promise to inform prospective parents on how to “mitigate more risks” and to take advantage of “life’s possibilities.” They offer to screen embryos for polygenic conditions such as heart disease, diabetes, and depression. “It would be crazy not to screen for these things,” has stated the founder and CEO of Orchid.
Clinically, PGT-P has limited accuracy and utility. And there are many concerns about entrepreneurs selling seaweed for silk ribbons or for supporters who embrace eugenics. But something else is the more serious problem hidden behind PGT-P: the folly of parents trying to achieve absolute control over their children. The technology promotes a very narrow idea of health and success and undermines the social conditions in which people utilize their capabilities.
[…]
However, supporters of PGT-P have no control, no matter how much they believe otherwise, when they try to select certain traits while rejecting others. Choosing the embryo with the lowest genetic risk for heart conditions and the highest potential for educational attainment may seem straightforward, but it is not. The portions of the genome that influence one complex trait also affect others. For example, selecting an embryo with slightly higher probabilities of educational attainment also means selecting an embryo with a 16% higher relative risk of developing bipolar disorder, according to a special report in The New England Journal of Medicine. And genetic research shows significant overlaps among the numerous genetic variants associated with autism and psychiatric conditions.
The company PGT-P Gattaca Genomics refers to the science fiction movie Gattaca, in which a character is born without the use of PGT-P and overcomes the odds that hinder his success. Another character who was born using the PGT-P method commits suicide when he does not live up to his genetic “destiny.” The movie teaches that expecting a child to have a genetic advantage can deprive individuals of something fundamental to human flourishing: the freedom to become who they are.
PGT-P is no longer science fiction. It is here, and the expectations it carries could be harmful to children, parents, and society. Emphasizing academic success alone does not lead to improved outcomes. In fact, constant focus on academic performance can cause harm to children. Children are more likely to thrive in school when they have the social structures of parental warmth and routine, and when they can discover who they are and be supported for their differences.
Parents who use PGT-P may claim that they can balance academic demands with social and emotional development, but this is not what the PGT-P selection decision promotes. On the contrary, it promotes the idea that parents can and should control variables that in reality are not always linked to future success or completion.
The social pressures exerted on modern parents to control what they cannot constitute a public health crisis. Doctors are ringing the alarm bell that 48% of parents experience anxiety that is “completely excessive” due to the impossible expectations around giving their child the best possible start in life. The increasing noise around PGT-P sends the opposite, and harmful, message: that health, success and happiness begin with genetics, parental control and optimization. On the contrary, PGT-P sets expectations that are impossible to fulfill.
Original title: Silicon Valley’s tech elite want to make superbabies. They shouldn’t.
Authors: Julia Brown,
Daphne Martschenko, November 23, 2024
Translation: Harry Tuttle