
The term “natural capital” was first used in 1973 by E.F. Schumacher in his book “Small Is Beautiful”1 and was further developed by Herman Daly2, Robert Costanza3 and other founders of the science of Ecological Economics, as part of a comprehensive critique of the shortcomings of conventional economics. “Natural capital” is a concept central to the economic valuation of “ecosystem services”4 which revolves around the idea that non-human life produces goods and services that are essential for life. Therefore, “natural capital” is necessary for the sustainability of the economy.
In a traditional economic analysis of the factors of production, natural capital is usually classified as “land”, a different concept from the traditional “capital”. The historical distinction between “land” and “capital” defined “land” as a natural phenomenon with fixed productivity, while “capital”, as originally defined, referred only to goods produced by humans, for example through agriculture. It is, however, misleading to consider “land” as if its productive capacity were fixed, since “natural capital” can be improved or degraded by human actions over time. Moreover, “natural capital” produces benefits and goods, such as timber or food, which can be harvested by humans. These benefits are similar to those realized by owners of industrial capital who produce more goods, and thus a factory produces cars just as an apple tree produces apples.
Ecologists have joined economists to measure and assess the values of ecosystem wealth as a way to find solutions to the biodiversity crisis. Some researchers have tried to put a dollar amount on global ecosystem services. If it is ecologically intact, the boreal forest5 has an estimated value of 3.7 trillion dollars. The boreal forest ecosystem is one of the planet’s largest atmospheric regulators, and stores more carbon dioxide than any other biomass on Earth. The annual value of the boreal forests’ ecological services is estimated at 93.2 billion dollars, or 2.5 times greater than the annual value of raw material extractions.
The economic value of the 17 services from ecosystems across the entire biosphere (calculated in 1997) has an estimated average size of 33 trillion dollars per year. These ecological economic values are not yet included in measurements of national incomes, GDPs, and do not have price determinations because they exist mostly outside global markets….
… The concept of “natural capital” has been used … in the Biosphere 2 project, and in the economic model of “Natural Capitalism” by Paul Hawken, Amory Lovins and Hunter Lovins… In their book Natural Capitalism: Creating the Next Industrial Revolution6, these 3 authors extend the concepts of capital beyond money and goods, to “natural capital” and “human capital”, arguing that the “next industrial revolution” depends on the adoption of four core strategies: “resource conservation through more efficient production processes; material reuse; changing the value assessment from quantity to quality; and investments in natural capital and the restoration/preservation of natural resources”.
…
In this “nature-friendly” way, Wikipedia presents the basic historical facts about the creation of the concept of “natural capital.” Or of the political idea that nature as a whole—all non-human life forms on the planet—is “capital.” The invention of “the economy of nature” (there are quite a few similar terms) can indeed be attributed to prominent figures of the ecological right as early as the 1970s; however, it is not difficult to understand it as part of “pan-capitalization,” the notion, that is, of everything as “capital” (and immediately thereafter as money), which is the core inspiration of neoliberalism. As such, this concept served as a response to the anti-capitalist tendencies of environmental movements, struggles, and actions of the 1970s and 1980s.
We will not continue with the topic of nature’s modern capitalism in general, although it is certainly important. It is an expression of the “general framework”. We are interested here in a subset: the idea of biological capital. Initially, this term referred to cultivated species, plants or animals, from the perspective of optimal capitalist exploitation. But it would not be possible for a concept with so many prospects for exploitation to be limited to fields, stables and farms; especially since “health” (in the human species) had been declared a basic component of “human capital” by the ideologues of neoliberalism.
As early as 1964, Gary Becker (who was quickly proclaimed the leader of the “third generation of Chicago School economists”) with his book Human Capital became the founder (initially marginal) of the idea that “health and education are investments in one’s own productivity,” and as such they should be treated: as the equivalent of any factory owner’s investment in new machinery.
In 1972 Michael Grossman, a student and fellow thinker of Becker, published his own doctoral thesis titled On the Concept of Health Capital and the Demand for Health. In the introduction he explained:
The purpose of this study is to construct a model for the demand for the commodity “good health”. The central hypothesis of the model is that health can be considered as a durable capital stock that produces outcomes. It is accepted that individuals possess an initial stock of health that loses its value over time and can be increased through investments. In this framework, the “shadow price” of health depends on many other variables beyond the price of medical care….
The dogma or “health is individual capital” began to become commonplace from the ’80s and, mainly, at a rapid pace from the ’90s onwards. But what is this so-called “health”? Not, of course, something abstract! Nor what each person subjectively feels! These vague and nebulous things cannot be measured; and if they cannot be measured, how can they be considered capital? The idea of “health capital” definitively erased the subjective perception of health or illness, completely removed or impoverished personality as the dynamic basis of social life, installing (or even imposing) a strictly measurable, mechanically “provable,” and statistically comparable list of records/registrations/indicators, from the moment of birth until the moment of death.
The biological capital, after its successful trials as “animal or plant capital”, was inevitably destined to expand and be applied (par excellence!) to the subordinates. With far greater demands, therefore with much greater ideological, political and technical complexity. In a related 2019 article, the value of bio-capitalizing the human species in general was indicated:
At the crossroads of sciences, epidemiology brings together the social and the biological… The idea of biological capital represents the accumulated history of biological experiences, along with other forms of accumulated capital, mainly cultural, economic and socioeconomic. The ability to access these three forms of private capital and, consequently, access to the appropriate position in life depends on inherited health capabilities, epigenetic influences and the accumulation of incorporated biological changes that make the individual more or less successful in life… We show that socially stratified conditions prior to illness, which are related to aging, can be controlled using biomarkers, in order to help underlying mechanisms promote healthy aging.
If health (and any illness) was pushed aside as personal experiences, as social issues, and as the presence or absence of symptoms; and if health was baptized as “capital,” this was not a change in secondary determinations. On the contrary, it was a Paradigm Change. Firstly, because for something to be characterized as “capital” it must be measurable by some “neutral” measure that would represent the “truth” while concealing its ideological components. And secondly, because the idea of “health capital” was the impetus toward extreme privatization, the individual “ownership” of health (of illness, of treatment), even though as early as the 1970s it was common belief that health (and illness) are multifaceted conditions, simultaneously individual and collective, and that healthcare is undoubtedly a social issue.
Nevertheless, although references to something proliferative or general (such as the “environment”) could occasionally be made in theories and discourses on biological capital, the foundation of the idea was privacy (of “biological capital”) and the perception of social relations as an aggregation of individual capitals, just as the market is the parallel display of concentrated commodities. This was/is capitalist bio-politics under neoliberal norms. So entrenched now that it seems difficult for one to realize that it is not only private bodies that suffer or thrive, but also their social relations; often primarily these.
immunocapital
The idea that immunity is “capital,” primarily individual, private, was not clearly articulated during the recent terror campaign. Nor did it appear as a specification of the broader and somewhat buried idea of (individual) “biological capital.” However, it was very specifically and strictly formatted with the vaccination passport or/and the immunity passport. The “passports” of vaccination or/and recent illness; the latter with an expiration date. It seemed “physiological” and anyway did not cause reactions: immunity became a crucial element of identity and, as such, a very valuable individual property, so valuable that it overrides (and dissolves) pre-existing social relationships.
We know that the EU was already preparing this kind of “vaccination passports” since 2018, and the fear campaign was a first, mass, general test. Both for their acceptance and for the technological specifications of the packaging. The justification in 2018 seemed innocent: “to know (the states, the public health officials…) who is in what condition – and to ban potential infectious individuals.” In 2018 and 2019, it seemed illogical to make extremely expensive preparations to shape the technical characteristics of a pan-European “vaccination passport,” since the only mandatory vaccinations to some extent or another were those for children. It was indifferent for 30, 40, 50, or 70-year-olds whether they had ever received… their childhood vaccines… against diphtheria and tetanus! And, of course, it seemed paranoid to impose restrictions on the movement of adults because… they missed some childhood vaccines!
After the sanitarian terror campaign we realized: it is not only the ever-multiplying children’s vaccines that are the issue. It is, above all, the lifelong artificial immunization (or what is sold as such), with repeated annual platforming; the permanent, ongoing surveillance of the general “biological capital” and especially the “immune capital,” based on the specifications of genetic engineering and pharmacomafia. Thus, before the term “immunity capital” was officially coined in 2020, 2021, and 2022, it had initially been nationalized, on behalf of the capitalist “health revolution.”
What was not done verbally with the appropriate formality (the declaration of immunity as capital…) by the terrorists, was done by Kathryn Olivarius in April 2020, retrospectively, in a critical way, with the pre-publication (in the establishmentarian New York Times) of a summary of her book (her doctoral thesis) Necropolis: Disease, Power, and Capitalism in the Cotton Kingdom which had not yet been published at the time7. This is a useful retrospective to the 19th century, and perhaps for this reason the carabinieri/Pfizer owners and directors of the New York Times did not consider Olivarius’s position “contaminated” or dangerous for the dominant dogma of 2020 and 2021, so they did not cut it. Fortunately.
The article was titled The Dangerous History of Vaccines8. Olivarius is an associate professor of history at Stanford. We translate below some interesting excerpts, and you will understand their relevance:
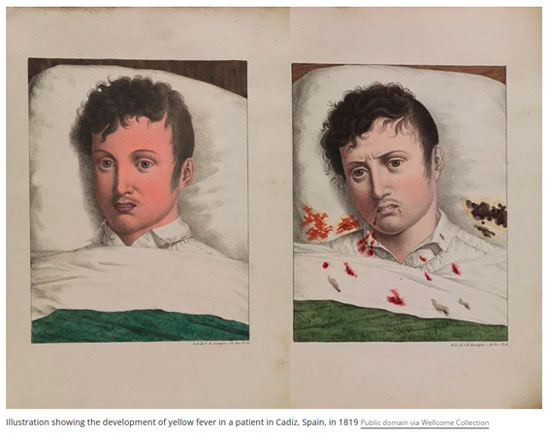
Yellow fever, a disease caused by a flavivirus transmitted by mosquitoes, was inevitable in the Deep South during the 19th century, and a subject of almost constant terror in New Orleans, the region’s hub. In the six decades that elapsed from the Louisiana Purchase from the French until the Civil War, New Orleans experienced 22 full-scale epidemics, which killed over 150,000 people in total. (Perhaps another 150,000 died in nearby American cities). The virus killed about half of those it infected, and killed them horribly, with many victims vomiting black coagulated blood, with the consistency and color of coffee grounds. The fortunate survivors had become “acclimatized,” or had acquired lifelong immunity.
Pre-war New Orleans was a slave society, where whites dominated over free people of color and slaves through legally sanctioned violence. However, another invisible hierarchy was combined with the racial one: white “naturalized citizens” were at the top of the pyramid, below them were white “non-naturalized foreigners,” and even lower were all others. Surviving yellow fever was locally called “baptism into citizenship”: proof that a white person was God’s chosen and was established as a legal and permanent factor in the Kingdom of Cotton.
Immunity mattered. “Unacclimatized” whites were considered unemployable. The German immigrant Gustav Dresel lamented in the 1830s: “I searched in vain for a clerk’s job” but “hiring a young man who had not acclimatized would cause nasty gossip.” Life insurers rejected related applications from unacclimatized individuals without a second thought, or otherwise charged them a very high “climate premium.” If someone was white, their state of immunity affected where they would live, how much money they would earn, whether they could obtain a loan, and whom they would be allowed to marry. It is therefore not surprising under these circumstances that many young immigrants actively sought to fall ill: they were crammed together in cramped accommodations or fell into a bed where acquaintances had recently died. They were the prewar ancestors of “pajama parties,” only yellow fever was far more deadly.
But immunity was more than just an epidemiological accident. In the context of the Deep South, it was used as a weapon. From the beginning, the wealthy white residents of New Orleans ensured that although mosquitoes treated everyone the same way, yellow fever would be anything but colorblind. Pro-slavery theorists used yellow fever to argue that racial slavery was natural, even humanitarian, because it allowed whites to maintain social distance from others; they could live in their homes, in relative safety, if blacks were forced to work and conduct trade on behalf of whites. In 1853, the newspaper “Weekly Delta” absurdly claimed that three-quarters of all deaths from yellow fever involved individuals who were against slavery.
Black people, with limited access to health care, were naturally afraid of yellow fever like anyone else. But slaves who gained immunity increased their monetary value for their owners by over 50%. In fact, the immunity of Black people became capital for white people.
It was not the yellow fever that turned the societies of the South into slave societies, but it widened the gap between rich and poor. The high mortality rate, as it turned out, was economically profitable for the most powerful citizens of New Orleans, since yellow fever kept wage workers insecure, unable to effectively negotiate increases in their wages. It is therefore no surprise that the city’s political leaders had no appetite to spend money from their tax revenues on disinfections, and instead supported the paradoxical view that the best solution to yellow fever was even more yellow fever. The burden of adaptation fell on the working class, not on investments by the rich and powerful in health infrastructure.
Olivarius speaks in her book about immunocapitalism; perhaps it would be more accurate to speak about immunofeudalism. The class structure of New Orleans, a former French colony, was “three-tiered”: at the top were the whites, in the middle the free people of color (“gens de couleur libres”), and at the bottom the black slaves. This stratification, before the American Civil War in which the industrial North imposed on the South the end of slavery because industries and factories could not implement the enclosure techniques of slaveholders, thus needing to hire free workers, can be considered pre-capitalist. Immunity invested this “three-phase” structure, inscribed in the feudal biopolitical power of white owners of vast cotton and sugar plantations in the American South: whites with immunity (the “naturalized”) acquired a freedom for all possibilities of social ascent, a “pass” in today’s terminology; free people of color with immunity could somewhat improve their position, within the limits of racial barriers; slaves with immunity simply became more “valuable,” merely enhancing the wealth of their owners.
The stratification of immune capital in Louisiana (although in the first half of the 19th century no one would use exactly this term) was also a management of morbidity. The masters of New Orleans called yellow fever “the sickness of strangers.” And they had the seemingly strange theory at first glance that Black people (slaves) could withstand it; or should be able to withstand it. Any new white European immigrants who had not acquired immunity were considered suspicious, useless, even dangerous; only by obtaining the early “immunopassport” of infection and survival could they be accepted into their freedom. In contrast, having a steady supply of slaves from Africa, white “acclimatized” masters believed that slave deaths were “divine will,” a kind of weeding out of the unfit for their plantations. In their own cosmoidol, the morbidity and high mortality of yellow fever, mainly at the expense of slaves, was what Darwin would later call natural selection – of a “lower” human species… For their own lines, in their houses, which were better protected from mosquitoes, roughly the same applied (“weeding out”) but rather as the inevitable price of business competition among themselves! It might be considered incredible (given today’s conditions, where morbidity, as we will see later, is mass-produced in a different framework), but the idea in racist New Orleans of the first half of the 19th century was that morbidity is functional, necessary, “productive.” That it contributes to the effective resolution of economic problems; and that the elite is unquestionable to the extent that it passes through illness and survives. (Of course, it is understood that there was no way to prevent yellow fever, except for mosquito nets on doors, windows and beds; something that was impossible for those living in caves, shacks and stables…) The “acclimatized” white feudal lords of the American South thus became, with divine blessing, the kings of cotton and sugar cane; and their immunity after infection was their crown.
the production of illness
The case of yellow fever in New Orleans was investigated, which is why we became aware of it through Olivarius’s analysis. We cannot know whether it was or was not unique. Its social and ideological characteristics should have been commonplaces throughout Christian slavery, but this is not enough for us to consider it not an exception but a model. In the end, it could be said that it concerns something very old, and has nothing to do with what we know from the 20th century onwards.
What do we know, however? The only certain distinguishing element of the New Orleans case is that it involved extensive contamination that was not anthropogenic. That is, it was neither the virus nor the contamination a deliberate human result/work. We know, on the other hand, and we know very well, that the development of the pharmaceutical industry has passed (and continues to pass) through “experiments”, contamination experiments, treatment experiments.
We know about the “medical experiments” of the Nazis in concentration / extermination camps during World War II… We know about the “medical experiments” conducted on thousands of prisoners by Japanese fascists from 1935 to 1945… We know that, in contrast to what happened to Nazi doctors (half of the total 15 were sentenced to death in the Nuremberg trials), equally criminal Japanese “experimenters” were granted amnesty by the American occupation general Douglas MacArthur, in exchange for handing over their findings to the U.S. (and some continued their research under a different regime…). We know about the “medical experiments” in American prisons in the 1960s and 1970s… We know about the “medical experiments,” described as “medical research,” conducted and still being conducted by Western “scientists” in Africa, Asia, and Latin America; even, as recently revealed, in Ukraine…
It would be the most foolish (and probably malicious) to attempt to characterize all these dense and extensive phenomena as exceptions. Or as “symptoms” of some ideological extremism (Nazis and Japanese fascists) which constituted an “unfortunate interruption” in what was otherwise a humanitarian, and particularly cautious and health-conscious, capitalist development.
Exactly the opposite is true. To the extent that drug production became industrial, subject to the iron capitalist “logic” of maximum profit, the organized production of illness (for decades to test the effectiveness of new drugs) became the most critical part of the production chain; of the R&D (research and development) departments of companies. What someone could claim as an “exonerating” argument in favor of the organized creation of illness for research (thus “good”) purposes, is that usually (with emphasis on the word “usually”) laboratory animals participate “voluntarily” – and are paid.
But can someone truly speak of “voluntary participation” in experiments that are dangerous? Obviously, people who are in great need of money put themselves on the butcher’s block; however, this is not “voluntary” except for the sake of appearances. Ultimately, to offer someone in prison that their sentence will be reduced or erased if they agree to become ill or even die is brutal blackmail. And of course there are countless cases where the organized production of illness for research purposes was carried out with the complete ignorance of the subjects that they were experimental animals.
It is inherent in the industrial phase of “health care,” essentially from the beginning of the 20th century if not earlier, the challenge of illness and/or pain in order to study A or B. An interesting and enlightening article with an even more provocative focus on the “value” of the deliberate production of morbidity, published in January 2021 in the “AMA Journal of Ethics,” under the title: How Should We Handle Information Gathered from Nazi Experiments?9 The author Arthur L. Caplan writes there:
The first time I encountered the issue of the morality of using information derived from heinous experiments was when I was teaching medical ethics at the University of Minnesota in the Twin Cities in 1988. I received an email from Robert Pozos, who was then a physiologist at the University of Minnesota in Duluth and particularly renowned as an expert on hypothermia. Pozos wanted my opinion on using information from experiments conducted by the Nazis at the Dachau concentration camp. The Nazi scientists, he told me, used 300 to 400 prisoners as human test subjects to find out how people survive or die under extreme cold conditions. They killed approximately 80 inmates by conducting research involving inhumane exposure to cold. The prisoners, mostly Poles and Russians, were submerged for hours in barrels of extremely cold water or left naked in the snow. Some died in order to draw conclusions about how much cold a human being can endure. Others were half-dead and then became test subjects for rewarming techniques (e.g., warm baths or body heat through embraces from female prisoners) to study the likelihood of resuscitation.
Pozos told me that his studies on human exposure to cold, funded by the U.S. Army and private companies operating in cold environments, had for years been conducted under the control of the funders and with the consent of the test subjects. The treatment for hypothermia available in the 1980s included extracorporeal blood circulation to warm the blood outside the body, warm air, and heated blankets. But Pozos’s studies on hypothermia had never approached temperatures that could kill or nearly kill human test subjects. Only the Nazis went that far, compiling the results in reports published in various journals, including the indictment at the Nuremberg trials.
Pozos thought that the information gathered by the Nazis from their experiments had value and warranted discussion, so we agreed to hold a conference at the University of Minnesota to examine when and how the information about hypothermia collected at Dachau would be used, and to reconsider the role of medicine in the Holocaust…
During the conference, we examined a discovery I made that the information collected at Dachau regarding human reactions to hypothermia had already been used by many armies of many states, including the United States. There were relevant reports in military circles immediately after World War II, during the national obsession with the alleged threat from the Soviet Union and preparations for a Cold War that could become hot (e.g., as happened with the war in Korea). Although I didn’t know it when Pozos approached me, I later understood that information considered by some to be helpful in case of war, in matters of national security or for dealing with terrorist threats, had already been deemed ethically acceptable to use, regardless of how it was obtained. This was the reasoning used by German scientists and doctors at the Nuremberg trials, as well as many others…
(This brief presentation does not at all deviate from the answer given by an American specialist (unfortunately we have missed her name) during the mass platforming of 2021, when she was told that threats and fines violate medical ethics as shaped by the Nuremberg trials. What was her answer? Well, the Nazis also helped advance science…)
Up to this point we have the extension of the purposiveness of producing illness (to the extent of pure torture chambers) from corporate research departments to military needs. It is not merely a quantitative expansion. But a qualitative one. Even if pharmaceutical companies could take refuge behind the argument that the illness they produce is limited and exclusively for “good purposes,” armies could not. The interest in Japanese illness production (to the point of amnesty for the fascists of Tokyo) and in the German / Nazi equivalent was / is nothing other than a few pages in the volume on biological warfare.
But pharmaceuticals cannot hide. In the course of the 20th century, they themselves took over the production of illness. An interesting study published in the British Medical Journal on April 13, 2002, is indeed outdated in relation to the achievements of the terror campaign of genetic engineering companies nearly 2 decades later, in 2020, 2021, and 2022, but it illuminates the immediately previous (to today’s) stage of this process. Under the title Selling Sickness: the pharmaceutical industry and disease mongering10 the authors Ray Moynihan, Iona Heath, and David Henry note:
Much money is made when you tell healthy people they are sick. Some forms of medicalization of everyday life would be better described as disease mongering: the expansion of the boundaries of treatable diseases in order to grow the market for those who sell and apply treatments. Pharmaceutical companies are actively involved in defining diseases, and promote these definitions both to those who prescribe the relevant drugs and to consumers. The social origin of diseases has been replaced by their commercial construction.
… Informal alliances have been formed between executives of pharmaceutical companies, doctors, and consumer groups across various disease categories. Although they appear on the surface to be focused on raising public awareness about health problems that have not been diagnosed or treated, these alliances present their own viewpoint as generalized, critical, and curable… A key strategy of these alliances is to target the media and, through them, with stories designed to create fear about condition X and draw attention to treatment Y. Consulting firms funded by the pharmaceutical industry supply the “independent experts,” consumer groups supply the “victims,” and public relations companies supply the media with the “positive” developments and various treatment “innovations.”
… In this article we do not intend to make a complete classification or definitive description of disease mongering, but rather to point out this serious situation that has not yet been properly assessed. We took examples from Australia, which are however internationally known, with five cases of disease mongering, which show specific aspects of this process: the characterization of common life events as serious medical problems; social problems that are baptized medically; mild symptoms that are presented as harbingers of serious diseases; common risks that are considered illnesses; and estimates of the prevalence of an illness that are inflated in order to create the idea of a significant problem…
It matters to recall the temporal/historical moment when the above text was written: in the early 2000s, of the 21st century. Consequently, it refers to developments already completed during the 1990s. And while it is easy for today’s reader to recognize in some of the above five specific processes of designed illness production certain dimensions of the terror campaign after 2020 (thus methods well-developed over at least 2 decades), a question could be posed: was there something at the end of the 20th century that favored the designed production of illness through propaganda, as identified in the early 21st century?
The answer is “yes”! It existed! And it is called acquired immunodeficiency syndrome – commonly known as AIDS. This is not the place to recount the history of AIDS and HIV. However, the data that subsequently proved to be a “source of inspiration,” as the above study describes, for the first major leap in constructing illness by pharmaceutical companies and their collaborators are certainly these:
Firstly, the great fear spread by the sexual transmission of this virus in sexually liberal Western societies for at least a decade, from the mid-80s onwards. Changes in behaviors in terms of “safety” certainly drew the interest of behaviorists…
Secondly, the fact that the HIV infection was (and could remain even for life) asymptomatic. There were no symptoms from the infection, neither immediately nor after a few days or even months. According to the officially accepted view, HIV attacks “silently” and slowly the T lymphocytes, which are a key element of the immune system. There are no symptoms of this syndrome itself, nor is it the direct cause of death. If someone exhibits symptoms that will be attributed to AIDS / to HIV infection, these will be from known infections or known cancers; which normally would have been dealt with by a competent immune system.
Third, the fact that for the first time in the western medical history, the capacity of natural immunity was recognized as a “target” per se. In the militaristic analogies related to the body and health (“viral invasions”, “defenses”, etc.), this was equivalent to a direct attack on the “headquarters”!
Fourth, the fact of asymptomatic cases placed individuals’ own perception in a secondary position, transferring the exclusive responsibility of diagnosis (via measuring T cell counts) to specialized tests, in laboratories, far from any direct experience. The first invisible “enemy” that could only be detected by the “radar of specialists” was not, of course, Sars-CoV-2 but HIV, in the 1980s… However, laboratories, tests and indeed the whole of laboratory medicine (which quickly began to generally and universally replace clinical medicine, diagnosis based on symptoms) were not and are not independent from pharmaceutical companies! The exact opposite is true: the chemical companies that make the laboratory equipment and consumables, and certainly set the specifications, criteria, the “standards” (of health or illness), are directly connected to pharmaceutical companies, which are also chemical industries. (Clinical) doctors have increasingly become components of this chain. Seminars, conferences, articles (and aggressive sales of specific “therapies”) are the means that keep these gears well-oiled.
Having ensured that it is a social belief that personal sensation is not only completely indifferent to whether someone is ill or not, but also probably dangerous (since it allows for complacency…); having ensured that “experts” are such not only in terms of treatment or diagnosis-of-illness-through-symptoms, but additionally are “experts in prognosis and prediction,” it was only a small step for the bosses of pharmaceutical companies to proceed to the trade of diseases (along with their treatments…), to the trade of risks (along with their precautions…). Initially in the way shown by the research of Moynihan, Heath and Henry: forging, exaggerating, intimidating an audience that had already definitively entrusted the management of personal/family “Health Capital” to third parties.
Selling Sickness has an interesting example of organized disease production – and let’s remember: we are only at the beginning of the 21st century, in 2002. The example concerns irritable bowel syndrome:
Irritable bowel syndrome is a common functional disorder, which until now only required confirmation of its benign nature. Now a campaign is being launched to repackage it as a serious illness, with a title and a drug, with all the consequences: costs but also serious side effects.
A confidential internal document that leaked from a medical publications company, In Vivo Communications, describes a three-year “medical education program” to create a new perspective on irritable bowel syndrome, that it is a “specific, common disease.” This educational program from 2001–2003 is part of GlaxoSmithKline’s promotional strategy for its drug Lotronex.
In Vivo is one of the few companies that openly specializes in “medical education” on behalf of pharmaceutical companies, and the leaked plan offers a rare opportunity to see the highly secretive world of drug promotion, with the new emphasis placed on “shaping” medical and public opinion regarding the latest diseases.
According to the documents, the main goal of the education program is this: «IBS (irritable bowel syndrome) must be put into doctors’ minds as an important and distinct disease condition». Patients should also «be convinced that IBS is a common and medically recognized disorder». The remaining issues concern the promotion of the “new clinically proven treatment” – Lotronex.
The first step of this process is to establish a “Consultative Committee, which will consist of a public opinion shaper from each state of Australia.” The main role of this Committee is to provide advice to the company’s goals for the current situation of gastroenterology and the “opportunities to be restructured.” Additional work should include “best practice guidelines” in the diagnosis and management of IBS and participation in international conferences. Another tactic is the production of an informational brochure before the circulation begins [of Lotronex] in order to “shape the market” and convince the “specialized market” that the condition is a “serious and real disease.”
For general practitioners, In Vivo suggests a series of advertisements in major medical journals, featuring interviews with members of the Advisory Committee that the company will (potentially) fund, because “their authority is invaluable in reassuring general practitioners that the material they receive is clinically valid.”
Other groups that will be targeted with advertisements include pharmacists, nurses, patients, and a medical institution described as already having a “close relationship” with In Vivo. A “patient support program” is also planned for 2002-2003, so that GlaxoSmithKline “secures customer loyalty to its own drug even when and if a competitor emerges.”
Although titled as a “medical education plan,” it is clear that this document serves as a promotional tool for Lotronex. A clause explicitly states that all publications from this specific campaign, including handwritten materials, must be approved by GlaxoSmithKline’s marketing, medical, and legal departments. The document also clarifies the significant role of the media, stating that “public relations and media activities are vital for a comprehensive campaign, especially in the area of consumer awareness”…
It is interesting what exactly GlaxoSmithKline intended to sell by transforming irritable bowel syndrome from a nuisance addressed with dietary caution into a “serious illness.” Treatment or disease? The answer came quickly when Lotronex was withdrawn before the “conquest of the Australian market” was completed and bore fruit, after the American FDA discovered serious and in some cases fatal side effects11.
the dialectic of power: artificial immunity, artificial illness
Michel Foucault in The Birth of the Clinic, reviewing analytically the birth, formation and establishment of clinical medicine at the end of the 18th and throughout most of the 19th century, indicates the politicization of bodies under the norms and specifications of the rising bourgeois class; a politicization that superficially enriches and expands the concepts of health and illness but at a deeper level binds them to an organic bipolarity, where something cannot be done (or conceived) for health without something being done (or conceived) for illness, and vice versa:
… The 19th century medicine … aligns more with normality rather than health; it shapes its concepts and defines its interventions in relation to a type of function or structure of the organism; and at the heart of every medical reflection … the knowledge of physiology will be installed, which was once marginal for the doctor and purely theoretical. Moreover, the prestige of the life sciences in the 19th century, their role as a model, especially for the human sciences, is initially not connected with the transferable and comprehensive character of biological concepts, but rather with the fact that these concepts were located in a space, the deeper structure of which corresponded to the opposition between healthy and pathological. When they speak about the life of groups and societies, about the life of the species or even about “psychological life,” they will think not only of the internal structure of the organized being but also of the medical bipolarity of normal/pathological. Consciousness lives, since it can be altered, mutilated, deviated from its course, paralyzed; societies live, since there are sick societies that wither away and others, healthy ones, in full bloom; the species is a living being that we see degenerating; the same applies to civilizations, the death of which we have observed so many times.
… Hence also the unique character of the human sciences, as they cannot indeed be detached from the negativity within which they emerged, but also relate to the positivity which they posit as a rule12.
Even if this was not originally a fundamental element of the urban idea of health and illness, bound together as they are, constantly moving back and forth, “justifying” each other institutionally, ideologically, scientifically (within or beyond quotation marks)—health justifying illness, illness justifying health—so that there could never be “complete health” if something, somewhere, somehow, could be pointed out as illness. Or if something could be indicated as a potential, as a likelihood of illness; something that, over time and through the exploitation of the idea of prevention, became much easier.
During the historical period of the birth of the clinic (late 18th, early 19th century – in France), as well as in feudal Louisiana (first half of the 19th century), the bipolarity of health – illness, which we could also call immunity – morbidity, had specific characteristics. In any case, it was symptomatic, and it was precisely this (: the symptoms) that constituted itself as a scientific body of knowledge with the birth and organization of clinical medicine. And in no case was illness (in Western societies) a human construct: there was still something like «God» or «fate» in human circumstances. (The tactic of deliberate biological warfare against the indigenous populations of North America during colonization, that is, the organized creation of deadly morbidity, was «exportable»…)13.
The bipolarity of immunity–disease (health–illness) has always been dynamic: it shaped social behaviors and practices, ideas, and state policies, and allowed for their periodic revision. Therefore, finding it in the industrial 20th century is not surprising.
Only now, the “production of health” is beginning to become a large-scale endeavor, thanks to advances in chemistry and the initiation of industrial drug production. And the “experimentation” for their efficacy gave another dimension to the already ideologically shaped bipolarity: along with industrial drug production and for the sake of their reliability for the sake of public health, there should be an entrepreneurially justifiable “margin” of controlled (experimentally) morbidity.
The “medical experiments” of the Nazi and Japanese fascists were not the manifestation of some ideological perversion. They were the (until then…) culmination of industrialism; the subjugation of the health–illness duality to industrial (Second Industrial Revolution) norms! That is why their findings, their conclusions (but also their methodologies) were eagerly adopted by the “forces of democracy and freedom” that won World War II, being equally industrial!!
By the mid-20th century, therefore, the chemical engineering of the health–disease dipole was shaped, as well as a certain social acceptance of it. A capitalist biopolitical “welfare” that guaranteed a decent (state) paternalism, whether for reasons of scientific progress or for reasons of military readiness. In Western societies, biological warfare appeared at the beginning of the century as “scientific fantasy” in stories by the American Jack London; during the First World War and, subsequently, the Second, research and tests became a tangible reality. But outside corporate and military laboratories, in “times of peace,” populations were not alarmed.
We identify the ground of serious developments in the management of the health–illness duality, as it was shaped under the title of the “welfare state” in the 1980s and 1990s. The “model change” has a name. It is called deregulation, started simultaneously in the USA (Reagan) and in Great Britain (Thatcher), and meant the gradual expansion of action margins on the one hand for pharmaceutical companies and on the other for insurance enterprises: the market liberalization14. Of “health services market”? That was the slogan, in a historical period where individual hygienism was becoming the banner of the Self–Capital, and of “health–capital.” But it would have been impossible to detach one pole (health) from the other (illness) in the organic, decades-old, mature duality! The political result of neoliberalism was not so much the “reduction of public health care expenditures due to competition” but, mainly, the transfer of the health–illness duality to a “higher level” of planning and applications. To the trade of morbidity—as we described earlier.
These, roughly, were the outcomes of the 1990s. Subsequently, it would be the biotechnologists/geneticists and their bosses who would take the place of the “driver.” There are numerous texts in cyborg literature on this topic, so we won’t provide references. However, we need to point out certain ideological “changes” that made possible yet another “level” in the complete subsumption of the health–illness duality under capital, reaching the point of mass bio-industrial production of sickness, rather than merely its commercialization.
An issue, “hidden in plain sight,” is who defines and how “public health” is determined. It is not only the second word that admits different definitions; it is also the first. Holocaust survivors, who recently witnessed from 2020 onwards the structural similarities or analogies between the recent campaign for the enforcement of genetic engineering and Nazi hygienic practices, correctly identified that determining who controls and defines the “public” (interest…) is of strategic importance. And not only in relation to health. They recalled that the concentration camps in Germany, even before the outbreak of World War II, when filled with “surplus” Germans, were justified in the public consciousness as measures for protecting public health. Since the determination of “public interest” is officially the responsibility of state authority and its institutional components, the “public interest” it invokes (or prohibits, or criminalizes) towards the individual members of a society is by definition suspect, if not dangerous. Even if it cites “public health” as its legitimizing principle. Perhaps especially when it comes to that: the moving bipolarity of health–illness lends itself to any kind of manipulation. And from this perspective, the spread of a certain social pathology (moral and emotional, primarily) is always possible—under the name of “protecting public health”: the extreme “lesson” of the second capitalist industrial revolution, whether from the Nazis or the Japanese fascists, was not (and could not be) an exception, an accident…
The acceptance of the idea of “Health – Human Capital” entrenched another toxic idea. Of the body as a fortress. Even though such representations existed earlier in a scattered manner, all the warlike/military metaphors of “siege” and “resistance” in relation to the health – illness duality began to gain ground already by the end of the 1970s, growing enormously in the following decades. AIDS provided an abstract representation for the “acropolis” of this fortress: the immune system. And the practitioners of genetic engineering settled there, to take care of (allegedly) the fortification works. In this way, what used to be the “exception” of peaceful life, namely the officially warlike/military management of the duality, began to emerge (initially ideologically) from the militaristic reserves.
Hygiene, this flag of the Self – Capital, began to fly high from the 1980s onwards. “Health – capital” became a cliché; it was a constantly expanding compromise with certain forms of illness, as evidenced by the almost proud proclamation of “I have a problem” (usually understood as “psychological”). Since no “castle” can be certain of being impenetrable, the obsessions with continuous health confirmation through measurements, tests, exams, etc., became a social norm; however, this “normalization” of what would once have been called hypochondriac behavior was simply the dark side of capitalization. “Capital” by definition (and) means destruction; creative destruction. What else could happen to bodies-as-capital except the agony of their “devaluation,” “underestimation,” “inability,” now understood in almost all capital forms, of money, fixed assets or/and commodities?
When, after 2000, genetic engineers began to display for commercial use what they intended to do, namely to “correct” the state of the health – illness dipole by tightening, loosening, replacing genes, this was already socially accepted as a conquest of invulnerability at its “source.” In the DNA. It was the useful illusion of fools. Even if the beastly health were artificially feasible, the severance as we might say of one pole from the other, the severance of health from illness, would be unthinkable from every angle under capitalist terms! It would be unthinkable from an economic perspective, from an ideological perspective, from a biopolitical perspective. The myths of immortality, incorruptibility, of “eternal youth” are exactly that: an armor of relations of exploitation and subjugation that massively produce death, decay, pain, sorrow.
Geneticists, biotechnologists, neuroscientists and their bosses spread the message that they are ready and willing to “solve all problems”, to eliminate every illness, to ensure for everyone “superior quality of life”, and so on. But what else would they say, if their techniques emerged for exactly the opposite reason? One of their sacred chalices is the natural immune system; not however to make the “castle” impregnable. But to undermine it in ways that are lasting and efficient. They want to finally conquer this last terrestrial continent in order to exploit it.
This is the historic moment when structural capitalist contradictions, the capitalist “creation-destruction” dipole, invest the cellular micro-scale of the “health-illness” dipole; it is the historic moment of “immunity-capital” and “sickness-investment.” The natural immune system must either be “blocked” or “bypassed,” in the name of treatment. It is considered “insufficient,” “incompetent” – perhaps even non-existent.
They say it as openly as possible.
On January 9, 2021 we wrote (unstoppable machine):
Ultimately, the bureaucracy of the I.M.F., as it operates as an agent in the service of the western bio-information-security complex, demonstrates its dangerous, anthropophagic absurdity.
A little over 10 days ago (Monday, December 28, mass bio-hacking!), we had presented the change in the definition of population immunity (herd immunity) on behalf of the organization… We will remind you of this change because there have been newer developments!
On June 9, 2020 the definition was this (from the official site of the “organization”):
Herd immunity is the indirect protection from an infectious disease that is achieved when a population has immunity either through vaccination or through immunity developed via previous infection.
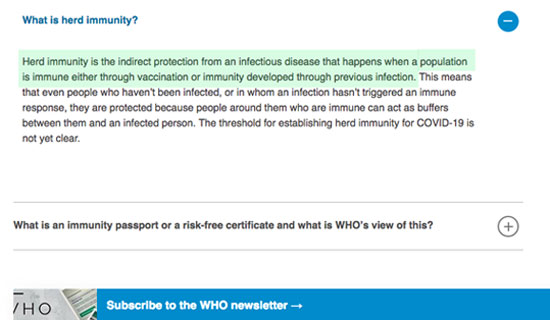
The definition was the known, established one for many decades – that’s why it was particularly brief. It wouldn’t teach anyone anything new.
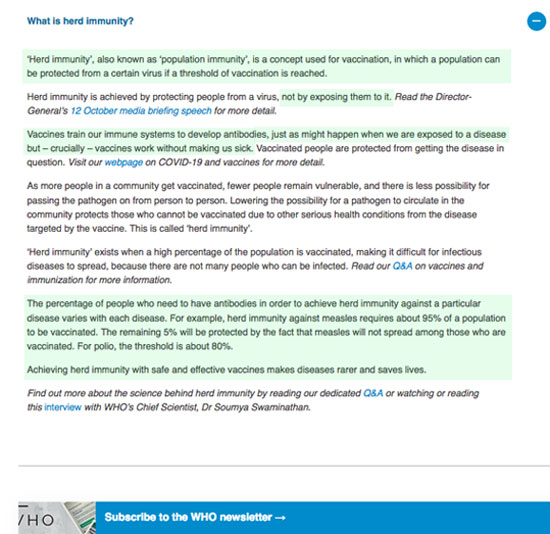
On November 13, 2020, the definition had changed radically. Natural immunity had completely disappeared, and the only “recognized” immunity was through vaccinations:
H “herd immunity” [note: this time in quotation marks…], also known as “population immunity”, is a concept used in vaccination, according to which a population can be protected from a specific virus if a vaccination threshold is achieved. Herd immunity [note: without quotation marks…] is achieved by protecting people from a virus, not by exposing them to it…
It was absolutely clear what this change served – and this is what we had indicated. Of course, neither the establishment demagogues nor the various lackeys and followers of the “hygienic recipe” of big pharma dealt with the issue.
However, at the end of 2020, the formulations of the definition were slightly altered, and the relevant reference grew even more; since, as it seems, even more “WHO arguments” must be given to the states and bosses who intend, at some point in the not distant future, to make the platforms compulsory…
What is the new thread of the bureaucracy bought by big pharma of the WHO?
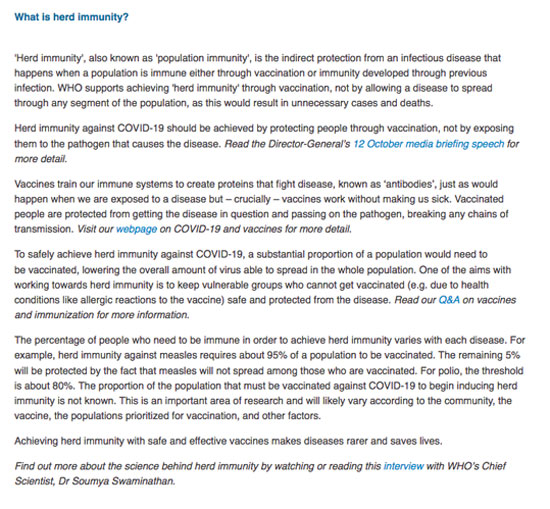
“Herd immunity,” also known as “population immunity,” is the indirect protection from a contagious disease that is achieved when a population has immunity either through vaccination or through immunity developed through prior infection…
Up to this point, it is a reproduction of the well-known, old and established definition as it existed on June 9, with the addition of the also well-known “population immunity” (there is still confusion with the herd?) and the quotation marks around the words herd immunity… And immediately afterwards, the downpour begins:The WHO supports achieving “herd immunity” through vaccination, not by allowing a disease to spread throughout the population, as such a thing would result in unnecessary cases and deaths. Herd immunity against covid-19 should be achieved by protecting people through vaccination, not by exposing them to the pathogen that causes the disease.
And it continues with a hymn to vaccines (that is, to genetic modification platforms), emphasizing that they do what happens naturally… but – and this is crucial – vaccines work without making us sick… In order to proceed to the other matter, the “percentage” of the population that needs to be platformized, citing selected examples of other diseases (95%, 80%…) so as to prepare the ground for compulsory platformization.
What happened and this silver-tongued bureaucracy was forced to upload a new patch with the “line”; We don’t know, but we can guess. The complete disappearance in November (from the definition) of natural immunity “bothered” the body so much as it is (a draft) that it was considered, probably, “counterproductive”!… It seems there were second thoughts, the relevant consultations took place, and the conclusion was to refer to natural immunity at the end of December, but only to characterize it immediately afterwards as problematic, dangerous, unacceptable – and “not permissible” by the WHO…. Perhaps as a remnant of a primitive era that has been overtaken by the civilization of genetic engineering.
The goal (and the result) is the same, as we described on December 28th. Natural immunity officially, persistently, and categorically enters the realm of illegality, along with the natural function and action of the human immune system! When natural immunity is accused (by whom? by the overlords who want to control our bodies…) as a “cause of increased cases and deaths,” the demagogues arm themselves to shout exactly that, not only regarding the tsahpini but, from now on, for every contagious illness, even the most common one, such as the flu!
Wait and sooner or later you will hear the parrots parroting the “correct line”! They will be demagogues, but they will also be doctors… (From those very few who feed at the stables of big pharma…)
On May 15, 2023 we completed:
…
Margery Smelinson, researcher and executive of the “store” headed by the proven unscrupulous Fauci, of the US “National Institute of Allergies and Infectious Diseases” / NIAID, decided to open her mouth by testifying before a subcommittee of the American Congress two days ago, which is investigating the “pandemic management.”The public health services of the USA, said Smelkinson, chose to downgrade natural immunity. How did they do this? Smelinson revealed that at some point in early 2021, Fauci, Rochelle Walensky (head of the CDC…), and other similar officials secretly met to see what they would do about natural immunity and, specifically, about the strong immunity following infection with the “common cold” virus, which threatened to blow up their entire campaign of violent platforming. The studies, serious and tiresome, one after the other in 2020 and early 2021 (presumably on “unvaccinated” individuals…) persistently showed (indicatively on the facing page) that the natural immunity of the vast majority of citizens (except those who already had poor health, as Chinese doctors had repeatedly shouted after Wuhan…) was doing just fine, not only against any infection but, moreover, after it.

The criminals had to answer whether infection and natural immunity due to equivalence counted “as one or more doses” of the mRNA platforms. Because thanks to their criminal ideology, natural immunity now had only one “measure”—the doses of the platforms; outside and far from these, there simply was no… It’s as if we’re saying: the natural immune system now existed only (and for as long as) the geneticists and other mafiosi permitted (and still permit…).
They decided to publicly announce that it’s not clear… it depends on each person separately… it’s unknown how long it lasts… And, ultimately, to order that for “safety reasons” everyone must take their doses, regardless of whether they caught it or not.
The downgrading of the natural immune system, essentially its proclamation, was a crucial ideological/political tool for legitimizing its mass dismantling by the general mechanics. It was a crucial ideological/political tool for exposing human bodies, embedding their inability before the alleged “new,” “unknown,” and “deadly” threat, and their voluntary surrender to genetic engineers and their masters. Genetics became instantaneously the TINA (: “there is no alternative”) for the leap into the norms of the 4th industrial revolution under the warm applause of thousands, millions of idiots. And the scum like Fauci and co. knew not only what they had to do but also how.
Some argue that the geneticists and their masters began the mass creation (in the name of “health”) of artificial immunodeficiency; a kind of genetic-aids, which is not transmitted from person to person, but is imposed by the conquerors of the “last continent”.
From an ethical perspective, it is terrifying. But from the perspective of capitalist SDI biopolitics for the 21st century, it is, unfortunately, “reasonable.” The “timeliness” of the biotechnologically guided displacement of the “health – illness” dipole toward the form of artificial immunity – artificial morbidity, if we can speak of something so hostile by calling it “timely,” lies in the following:
Firstly, in that the Change of Paradigm and the adaptation of (Western, of course) populations to the norms of the 4th industrial revolution CANNOT be done “with kindness,” that is, with the “freedoms” that were sold as the trademark of the neoliberal capitalist period 1980 – 2010. It must be done through violence, because it concerns abrupt, radical changes in basic and crucial (daily) behaviors. In cyborg 18 we presented certain documentation of this (Western) capitalist necessity for violent transformation of social relations15.
Secondly, in that this violent (and fast) transformation of social relations cannot but be simultaneously “at the heart” of the fantasies of the masses of citizens and profitable for business sectors that are “technological champions” of Western capitalism. Biotechnologies are the last such sector remaining in competition with Chinese / Asian / Eurasian capitalism.
Third, in that the health check of citizens is a check of everything. Of production/productivity, of consumption/consumerism… The Western masters would like this “everything” to include the entire planet, but… no… They are limited to the current historical circumstances in the territories of their own states and some (not definitive) allies of theirs, concentrating “technological fires.”
Fourth, in that organized illness production is the only profitable and invasive way to control-health, that is, to control-everything, penetrating the soft underbelly of the belief in individual/family “Health-Capital.” The dialectical synthesis of health-illness is now called functionality. Which means to be sick but, at the same time, to be functional with respect to “purposeful,” that is, capitalistically exploitable, everyday activities.
Fifth, in that the organized production of morbidity fits and serves both the military research and purposes of biological warfare – which should now be considered part of the daily agenda.
Indeed, the technological alienation of the natural immune system is the avenue for the liquefaction of the “health – illness” duality.
It’s not a few things..
Ziggy Stardust
- Full title: Small is Beautiful: A Study of Economics As if People Mattered. It was published in Greek in 1980 by the publishing house “Glaron”, with the accompanying comment “The small is beautiful” opens the way for a world where Capital will serve Man, overturning the current situation where Man remains a slave to Capital.
What did you say? ↩︎ - American economist and ecologist, academic who served as a senior official of the World Bank from 1988 to 1994… ↩︎
- American-Australian ecological economist, university professor… ↩︎
- Tertiary education in all its glory… ↩︎
- “Boreal forests” (or taiga) are the coniferous forests located above the 50th parallel in North America and Eurasia. ↩︎
- It was published in 1999, and has been translated into over 10 languages. ↩︎
- It was published by Harvard University Press in early 2022. ↩︎
- Fully behind a paywall at https://www.nytimes.com/2020/04/12/opinion/coronavirus-immunity-passports.html ↩︎
- Accessible at https://journalofethics.ama-assn.org/article/how-should-we-regard-information-gathered-nazi-experiments/2021-01 ↩︎
- Accessible at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1122833/ ↩︎
- The authors refer to 2 links with the relevant FDA announcements… which have now been “taken down”. Obviously, the “responsible guardians” have learned over these years, from 2002 to 2023, to be more “friendly” towards their bosses… More “careful” about what they allow to remain in cyberspace… ↩︎
- Ch. 2, A Political Conscience, pp. 69–70 ↩︎
- Indicatively: Did Colonists Give Infected Blankets to Native Americans as Biological Warfare? available at https://www.history.com/news/colonists-native-americans-smallpox-blankets ↩︎
- This “liberalization of the health market” did not go unnoticed. However, it was conceived in a very narrow way, as a “parenthesis” that could simply be reversed. The fact that it involved the liberalization of capital and the fact that capital in the late 20th century was multi-layered, relational, “social” and dynamic was either ignored or misunderstood. ↩︎
- Cyborg 18, June 2020, The shape of things to come. ↩︎